Hi Damon
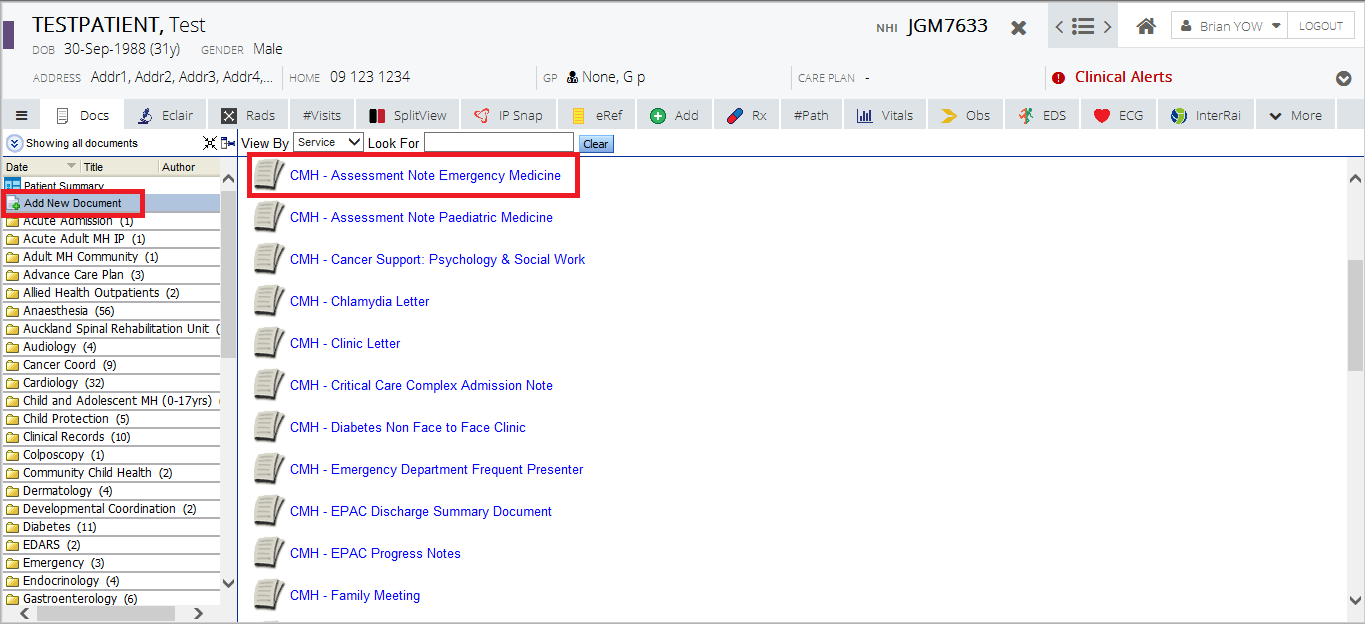
In ED we did it with SMT adhoc, as some clinicians still prefer to do it on paper. The adhoc avoids the encounter number issue and it’s completely optional. The other specialties e.g. Gen Med, OPH, med subspecs we did it with the episode linked SMT. There’s different SMT rules and limitations for things like pre-populating for adhoc vs episode linked, so pros and cons
Overall something like 90% are electronic now, was a gradual conversion rate. Basically all the night staff find it easier to handover electronically, everyone can read it at handover/postacutes/legibility/visibility etc
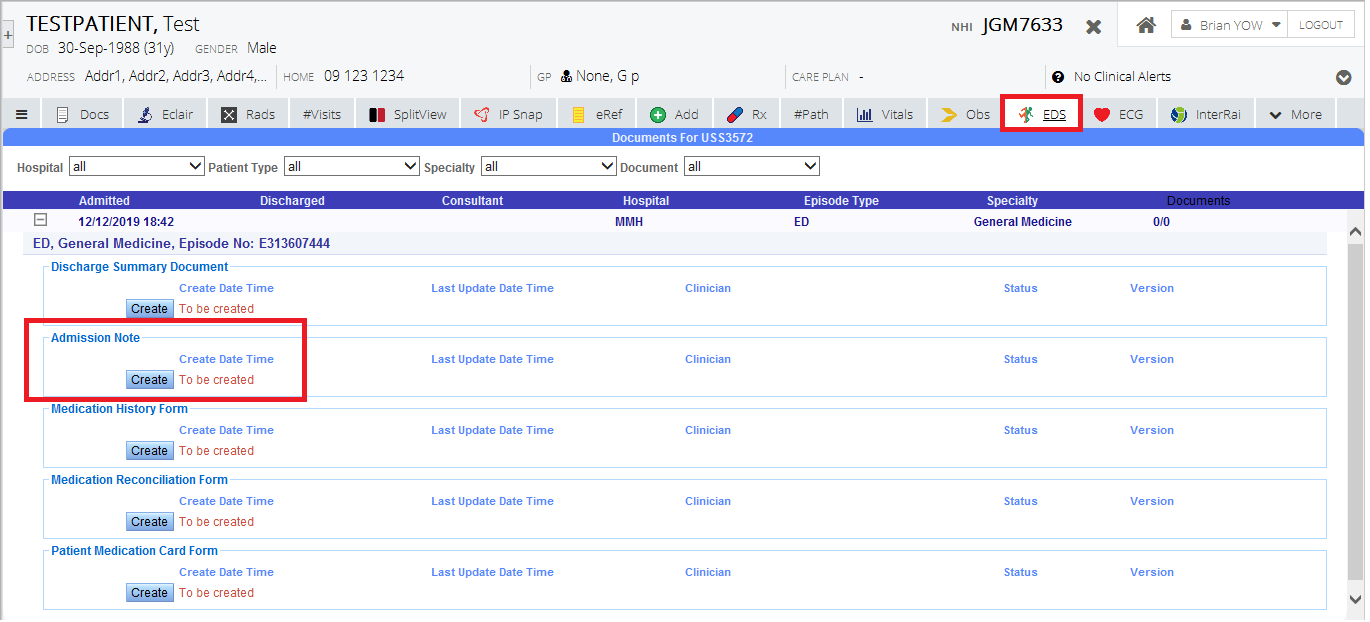
You are right there are some things to work through with the iPM encounter numbers (our PAS), transfers from ED to other departments can cause issues sometimes
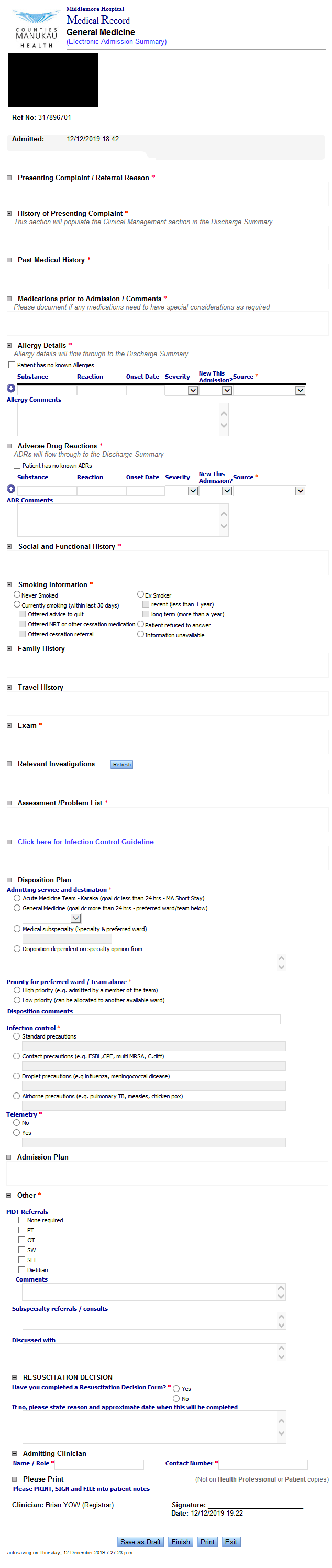
Our ED guys are now asking to remake their admission note and look at doing a streamline data flow populating from A-to-D from ED to Gen Med to OPH for example - maybe we can have more functionality doing this with Care Pathways instead
We haven’t done it in Surgical specialties due to faster workflow, only doing it now starting in Ortho. WDHB have implemented it for all specialties I think
You are right there are definitely ‘copy and paste’ syndrome problems with pre-populating. The balance is whether we want busy admitting clinicians to have nothing vs something to start with
Although I think (perhaps naively) this would improve if we did implement end to end electronic notes, including inpatient consults, progress notes, Ward rounds etc. If people see the value and the majority try to at least glance through it and update it a little bit then it might reach critical mass and stay reasonably accurate/current
Although we are still missing GP (we don’t have HealthOne) and of course the patient (can’t wait until we finally get a patient portal) so there are significant gaps
We are also looking at the Orion Read/Write/Reconcile Problem List that has 2 way population with Care Pathways. So then the PL might become source of truth and that surfaces in every admission, EDS, clinic letter, ward round note etc. Then at least it is visible at various points of clinical workflow to encourage people to look at/update it at multiple points of care
There’s a regional discussion occurring re Problem List (both the concept and the Orion application) and data strategy/architecture. @jenp our Counties Programme Manager and @Tina.Sun Clinical Director IS sit on HSDC Health Services Design Council where this is tabled and will be valuable to get their input. @lara is on that from WDHB side and she has always been a key pillar for Clinical Informatics in the region