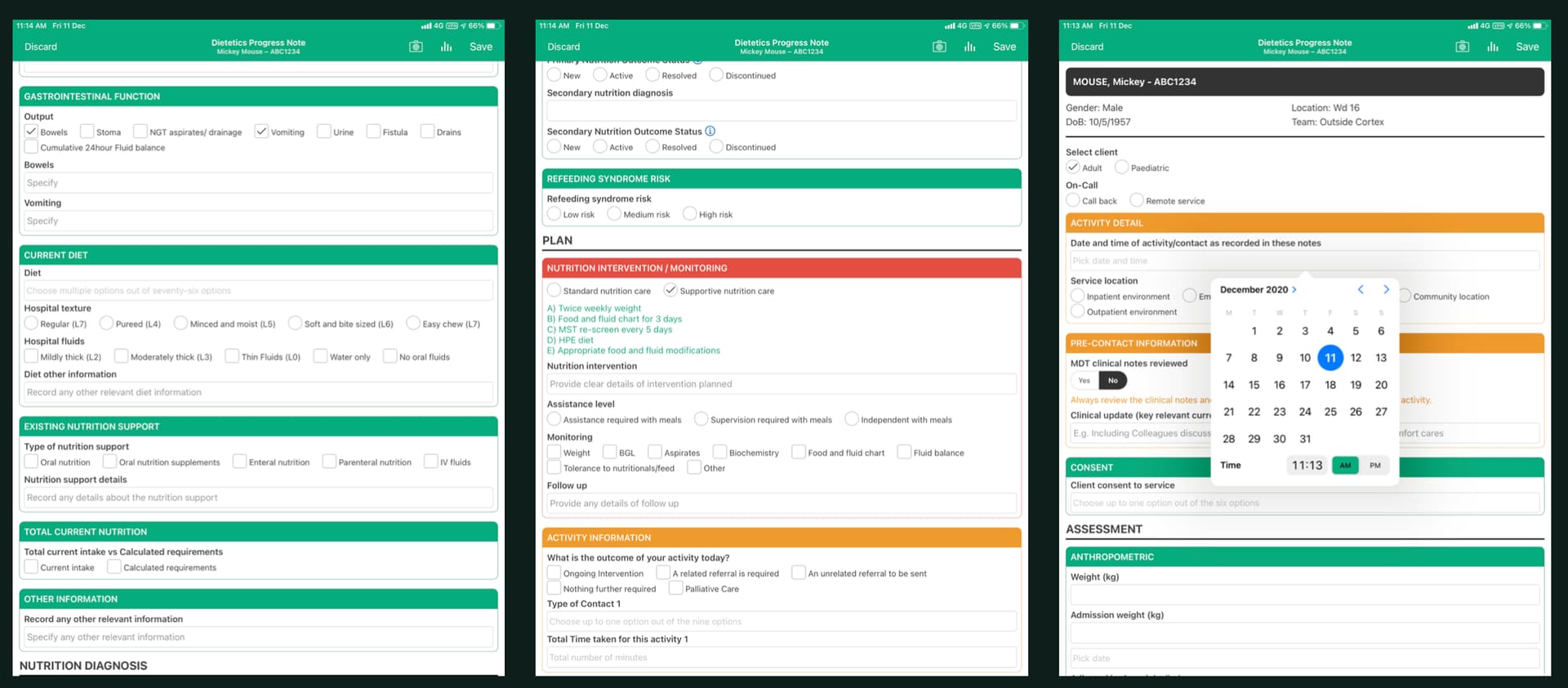
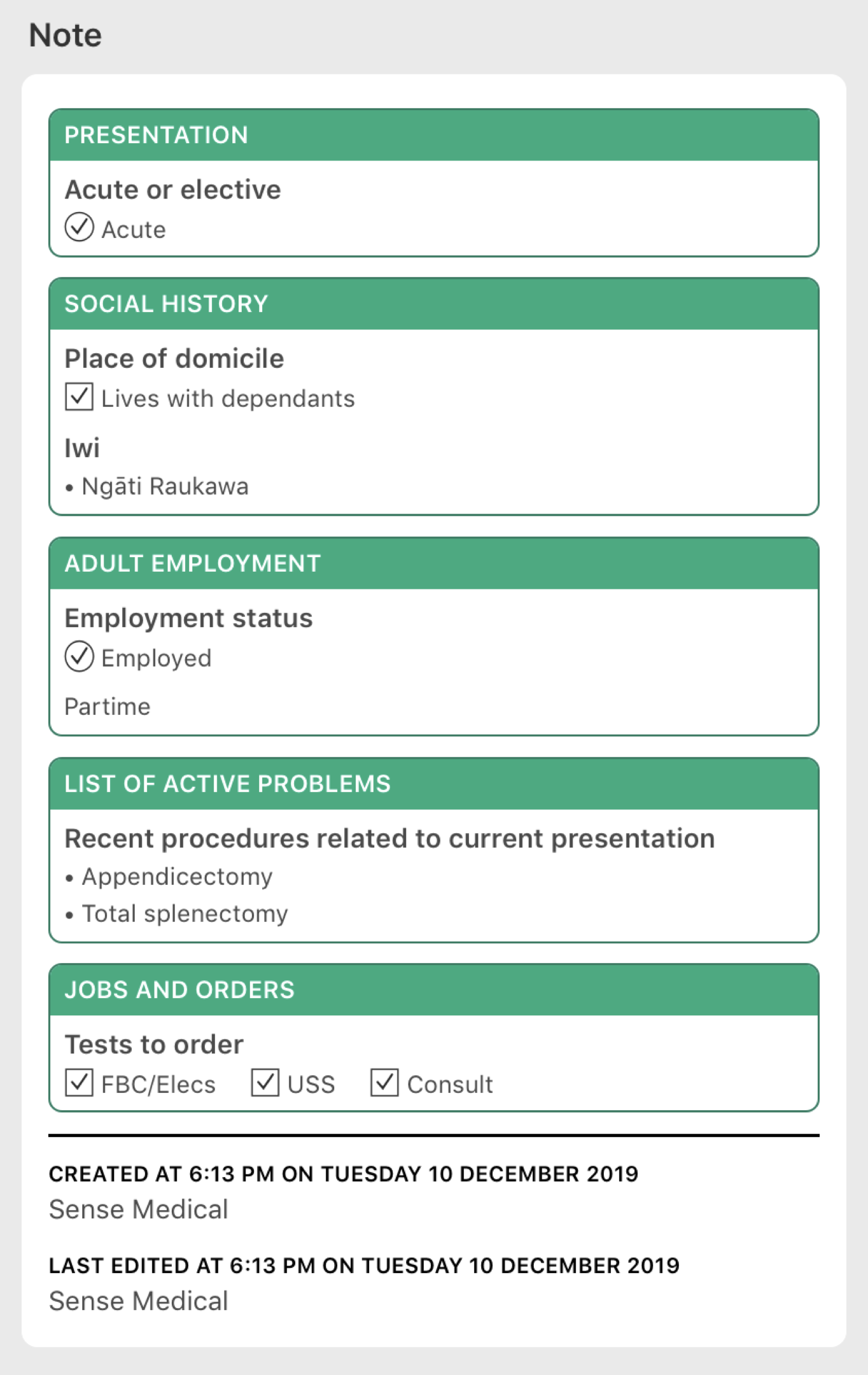
There’s quite a focus on forms here - clearly the evolutionary stage we’re at (mostly). I think one of the challenges we need to focus on is data retrieval. Forms are an obvious mechanism for data capture, but at present, we’re more or less locked in to viewing/retrieving data in the form it was captured in.
We’re still often only digitising paper (as artefacts of various clinical processes). There’s significant duplication/replication across these forms given each tends to be developed as an individual piece of work. Many of the person-level elements, ubiquitous across most forms, are not yet centrally stored or managed in a usable way, and as such, each form is often a snapshot/silo, only viewable by opening that form. In the wider context (i.e. including non-inpatient areas), medications, alergies and alerts, conditions/diagnoses, medico-legal, family violence screening, smoking cessation, personal preferences/needs/supports, dependents etc are all aspects of person-level information routinely captured in silos across a multitude of forms. Further, we have an over reliance on finding (in our digitised paper file) and opening discharge summaries as our main source for previous history. We have limited local contextual views of information able to be generated from data captured across our array of forms, let alone any person-level equivalents available wherever a person may present.
Smoking cessation is an interesting one. There is a national requirement to capture and report these data, along with national guidance around when and what is to be captured, yet like many such things, interpretation and variation has pervaded. Standards are only part of the solution, with the main issue being multiple repositories of the same person-level data (at a form level, application level, provider level, district level, regional level - depending on the service location). Interoperability is also only part of the solution, as this suggests being able to exhange data between silos in a standardised way. Obviously this is critically important, however in the case of many of the elements noted previously, reducing the silos - and in fact, establishing core repositories of commonly utilised data would seem like something we should be aiming for.
I agree that sharing ideas and examples would be great - particularly specific aspects around data integration, management and retrieval. I’m not sure there’s huge value at this point in sharing forms, given that array of tools and subjective content variation that exists.